Many patients search online for sulfa allergy safe drugs after experiencing severe reactions to antibiotics such as co-trimoxazole (trimethoprim-sulfamethoxazole). When people hear the term “sulfa allergy,” confusion often follows. Some patients wonder if they must avoid every drug with “sulfa” in the name. The truth is: not all sulfa-containing medications are dangerous. The key is understanding the chemical structure—specifically whether the drug contains the N4 arylamine group.
The Real Culprit: The N4 Arylamine Group
The allergy risk in sulfonamide antibiotics comes from a specific chemical feature known as the N4 arylamine group. This group is highly immunogenic, meaning it can trigger a severe immune reaction, such as Stevens-Johnson Syndrome (SJS) and Toxic Epidermal Necrolysis (TEN).
The sulfonamide scaffold itself is not the problem. It’s the presence of the N4 arylamine group that makes a drug high risk.
👉 So the better question isn’t “Is this drug a sulfa?” but rather: “Does this drug contain an N4 arylamine group?”
Why Avoid Sulfasalazine and Dapsone?
Sulfasalazine: While not an antibiotic itself, it is metabolized into sulfapyridine, an arylamine sulfonamide antibiotic. That means it carries the same high-risk N4 arylamine structure.
Dapsone: Technically a sulfone (not a sulfonamide), but it still contains an N4 arylamine group. Immunologically, it behaves like sulfonamide antibiotics and poses a similar risk.
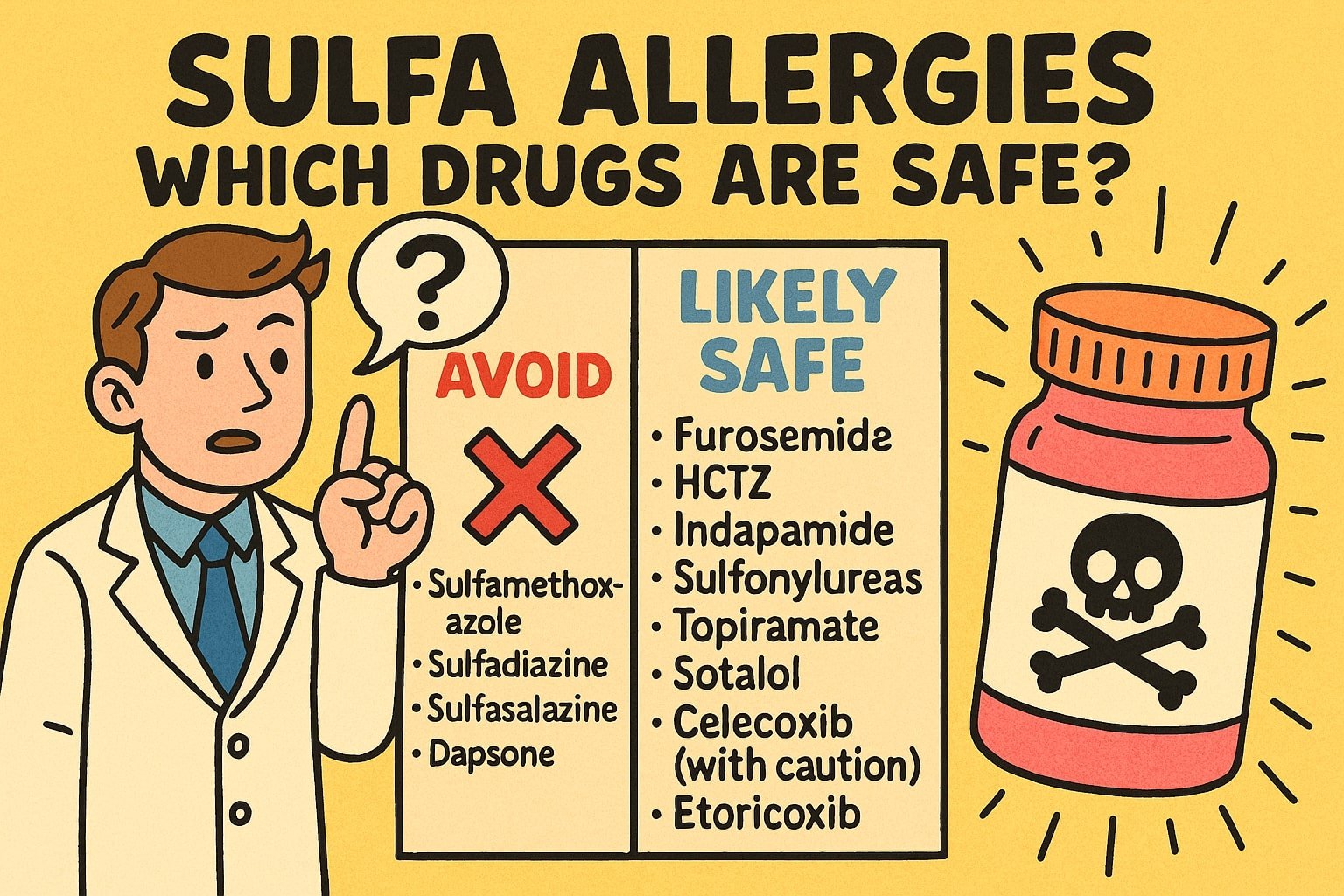
Sulfa Allergy Safe Drugs vs. High-Risk Drugs ✅
Most non-antibiotic sulfonamides do not contain the N4 arylamine group. These medications are considered sulfa allergy safe drugs, with no expected cross-reactivity:
- Diuretics: furosemide, bumetanide, thiazides (HCTZ, indapamide, chlorthalidone)
- Diabetes medications: sulfonylureas (glipizide, glyburide, gliclazide)
- Others: topiramate, sumatriptan, sotalol
⚠️ Note: These drugs can still cause unrelated allergic reactions, but not due to sulfa cross-reactivity.
What About COX-2 Inhibitors? (Celecoxib and Etoricoxib)
This group deserves special mention.
- Celecoxib: Contains a sulfonamide group but no N4 arylamine. It’s generally safe in a sulfa antibiotic allergy but has been rarely linked to its own, independent cases of SJS/TEN (de novo reactions).
- Etoricoxib: Has a sulfonyl pharmacophore, not a sulfonamide. It has no N4 arylamine group and is safe in sulfa antibiotic allergy.
Cross-reactivity Rare cases of patients reacting to both celecoxib and etoricoxib have been reported. This is likely due to a shared part of their structure called the COX-2 diaryl–sulfonyl pharmacophore. This is completely unrelated to sulfa cross-reactivity. If you are allergic to celecoxib, you should avoid etoricoxib.
Quick Reference Guide for Sulfa Allergy Safe Drugs
| Drug Class | Examples | Safe After SJS/TEN from Sulfa Antibiotic? | Why? |
| Sulfonamide Antibiotics | Sulfamethoxazole, sulfadiazine | ❌ Avoid | Contain N4 arylamine |
| Sulfasalazine | — | ❌ Avoid | Metabolized to sulfapyridine (an arylamine) |
| Dapsone (sulfone) | — | ❌ Avoid | Contains N4 arylamine |
| Non-arylamine Sulfonamides | Diuretics, sulfonylureas, topiramate, sumatriptan, sotalol | ✅ Safe | No N4 arylamine |
| Celecoxib | — | 🟡 Safe with caution | No arylamine; rare de novo reactions |
| Etoricoxib | — | ✅ Safe | Sulfonyl structure; no arylamine |
| Celecoxib ↔ Etoricoxib | — | ⚠️ Rare cross-reactivity | Shared COX-2 pharmacophore |
Export to Sheets
Personal Insight and Nuances
While the theory is clear, real-world practice shows that not all sulfonamide antibiotics or dapsone exposures result in cross-reactivity.
- Dapsone cross-reactivity: Studies suggest cross-reactivity rates between sulfonamide antibiotics and dapsone can range from 10–20%, depending on the population studied (higher in HIV-infected patients).
- Individual variability: We’ve seen patients allergic to sulfadiazine who later tolerated sulfamethoxazole under a graded challenge after negative in vitro testing. Still, the standard recommendation is to avoid alternate sulfonamides unless absolutely necessary.
- Phenotype matters: This discussion applies mainly to T-cell–mediated, non-immediate reactions (e.g., DRESS, SJS/TEN). Cross-reactivity in IgE-mediated immediate reactions (like urticaria or anaphylaxis) may follow different patterns.
FAQ
Q: What are the sulfa allergy safe drugs I can use?
A: Most non-antibiotic sulfonamides (such as thiazide diuretics, furosemide, sulfonylureas, topiramate, sumatriptan, and sotalol) are considered sulfa allergy safe drugs because they lack the N4 arylamine group.
Q: Do I need to avoid dapsone if I’m allergic to etoricoxib?
A: No. Cross-reactivity is not expected. Dapsone contains an N4 arylamine; etoricoxib does not. Their risks are unrelated.
Q: Can I take diuretics if I have a sulfa allergy?
A: Yes. Diuretics lack the N4 arylamine group and are generally safe in patients with sulfa allergy. They may still cause unrelated allergic reactions.
Q: Is celecoxib safe in sulfa allergy?
A: Usually yes. Celecoxib does not have an N4 arylamine group. Rarely, it has been linked to independent SJS/TEN, but this is not due to sulfa cross-reactivity.
Q: Why is sulfasalazine risky in sulfa allergy?
A: Because it is metabolized into sulfapyridine, an arylamine sulfonamide antibiotic, which carries the high-risk N4 arylamine structure.
⚠️ Disclaimer
⚠️ This blog is for educational purposes only. Severe drug allergies such as SJS/TEN should always be managed by an allergist or a qualified specialist. Do not start or stop medications without medical advice.
References
- Strom BL, Schinnar R, Apter AJ, et al. Absence of cross-reactivity between sulfonamide antibiotics and sulfonamide nonantibiotics. N Engl J Med. 2003;349(17):1628-35.
- Brackett CC, Singh H, Block JH. Likelihood and mechanisms of cross-allergenicity between sulfonamide antibiotics and other drugs containing a sulfonamide functional group. Pharmacotherapy. 2004;24(7):856-70.
- Slatore CG, Tilles SA. Sulfonamide hypersensitivity. Immunol Allergy Clin North Am. 2004;24(3):477-90.
- Ponce V, Muñoz-Bellido F, Moreno E, Laffond E, González A, Dávila I. Fixed drug eruption caused by etoricoxib with tolerance to celecoxib and parecoxib. Contact Dermatitis. 2012;66(2):107-8.
- Shah TJ, Moshirfar M, Hoopes PC Sr. “Doctor, I have a Sulfa Allergy”: Clarifying the Myths of Cross-Reactivity. Ophthalmol Ther. 2018 Jun 29;7(2):211-215. doi: 10.1007/s40123-018-0136-8. PMID: 29959752; PMCID: PMC6258578.